Type 2 Diabetes Mellitus
Summary
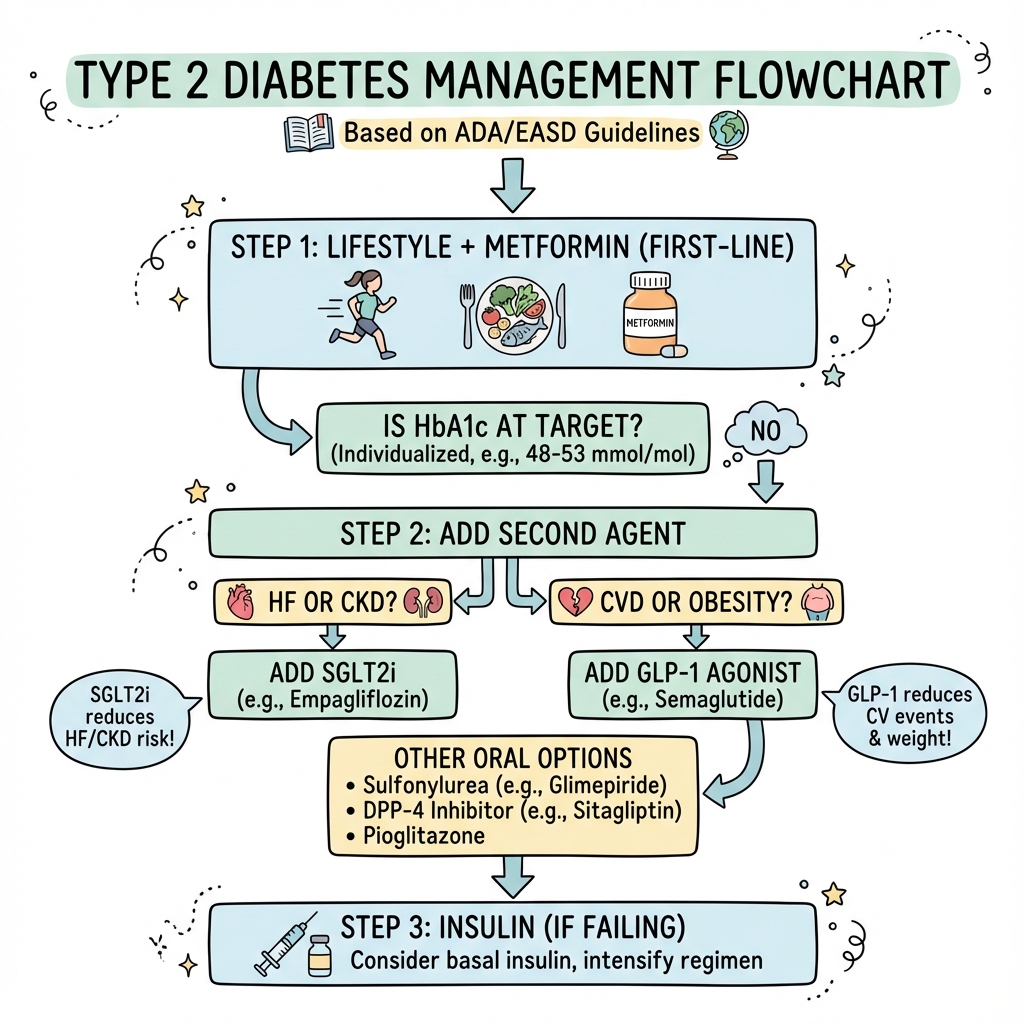
Type 2 diabetes is a metabolic disorder characterised by insulin resistance and relative insulin deficiency. It is the most common form of diabetes. Management is stepwise: lifestyle modification + metformin first-line, then add SGLT2 inhibitor (if CKD/HF) or GLP-1 receptor agonist (if CVD/obesity). Cardiovascular risk management is integral. HbA1c target is individualised (typically 48-53 mmol/mol).
Key Facts
- Definition: Insulin resistance with progressive beta-cell failure
- Incidence: 400+ million worldwide; increasing
- Pathognomonic: Hyperglycaemia + HbA1c 48+ (6.5%+)
- Gold Standard Investigation: HbA1c, fasting glucose
- First-line Treatment: Lifestyle + metformin
- Prognosis: Good with multifactorial management
Clinical Pearls
SGLT2 Pearl: SGLT2 inhibitors protect kidneys and reduce heart failure independently of HbA1c.
GLP-1 Pearl: GLP-1 agonists reduce CV events and promote weight loss.
Target Pearl: Individualise HbA1c target - 48 for most, higher if frailty/hypoglycaemia risk.
| Test | Diabetes |
|---|---|
| HbA1c | 48+ mmol/mol (6.5%+) |
| Fasting glucose | 7.0+ mmol/L |
| OGTT 2h | 11.1+ mmol/L |
Algorithm
Stepwise Treatment
| Step | Options |
|---|---|
| 1 | Lifestyle + Metformin |
| 2 | Add SGLT2i (CKD/HF) or GLP-1 (CVD/obesity) |
| 3 | Triple therapy or insulin |
Drug Classes
| Class | CV/Renal Benefit |
|---|---|
| SGLT2 inhibitors | HF, CKD protection |
| GLP-1 agonists | CV event reduction, weight loss |
| Sulfonylureas | Low cost, hypoglycaemia risk |
| DPP-4 inhibitors | Neutral |
-
ElSayed NA et al. Standards of Care in Diabetes - 2024. Diabetes Care. 2024;47(Suppl 1):S1-S321.
-
NICE guideline NG28. Type 2 diabetes in adults: management. 2022.
Viva Points
"T2DM: metformin first-line. Add SGLT2i if CKD/HF, GLP-1 if CVD/obesity. SGLT2i protects kidneys and heart. Individualise HbA1c."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team