Mixed Connective Tissue Disease
Summary
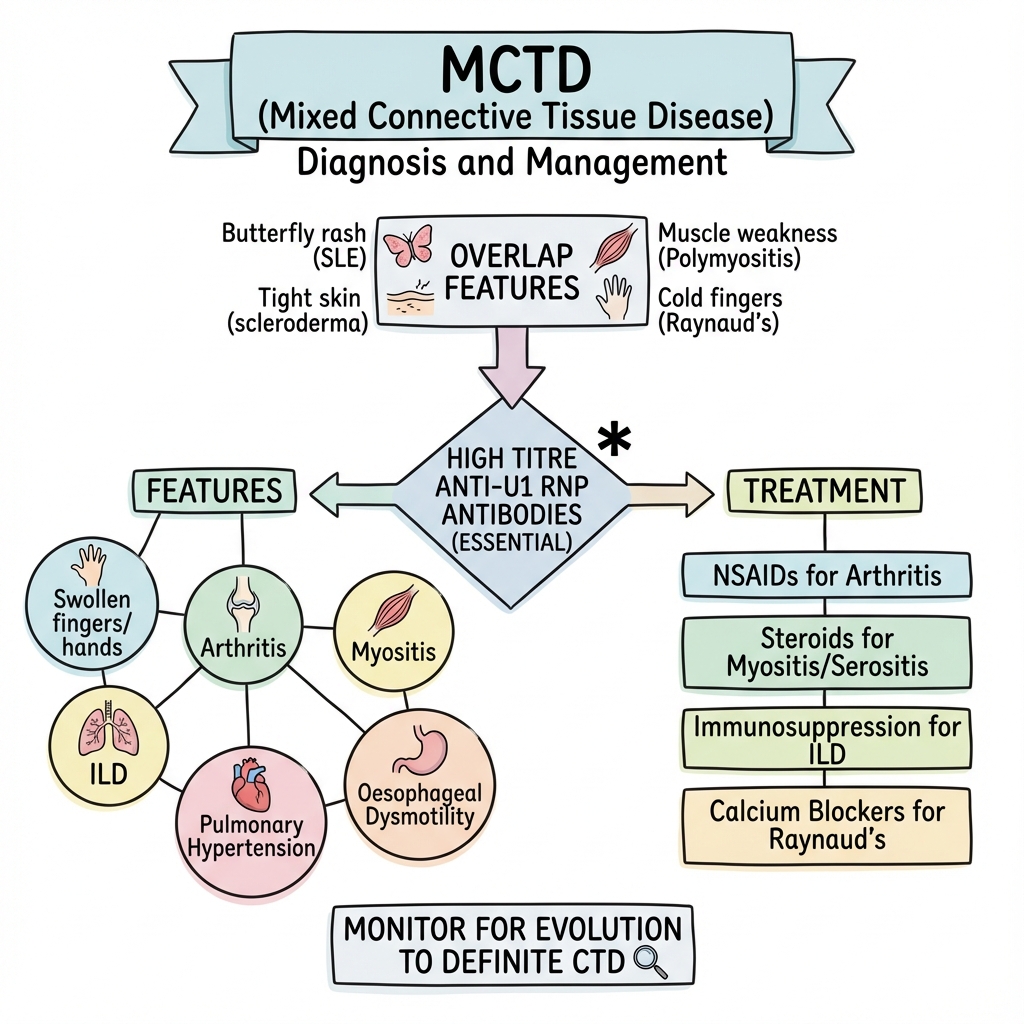
Mixed connective tissue disease (MCTD) is an overlap syndrome with features of SLE, systemic sclerosis, and polymyositis, associated with high titres of anti-U1 RNP antibodies. First described by Sharp in 1972, it is characterised by Raynaud's phenomenon, swollen hands, polyarthritis, myositis, and internal organ involvement. Pulmonary arterial hypertension (PAH) is the most serious complication. Some patients evolve into a definite connective tissue disease over time. Treatment is symptom-directed.
Key Facts
- Definition: Overlap CTD with anti-U1 RNP antibodies
- Incidence: 2-10 per 100,000; F greater than M 9:1
- Peak Demographics: Women 30-50 years
- Pathognomonic: High titre anti-U1 RNP + overlap features
- Gold Standard Investigation: Anti-U1 RNP antibodies
- First-line Treatment: Symptom-directed; steroids for myositis/serositis
- Prognosis: Variable; PAH major cause of mortality
Clinical Pearls
Diagnostic Pearl: Anti-U1 RNP must be present at high titre for MCTD diagnosis.
Complication Pearl: PAH can develop years after diagnosis - screen with echo.
Evolution Pearl: 30% evolve to definite SLE, scleroderma, or other CTD.
| Feature | Frequency |
|---|---|
| Raynaud's phenomenon | 95% |
| Swollen hands ("sausage fingers") | 90% |
| Polyarthritis | 80% |
| Myositis | 50-70% |
| ILD | 50% |
| Oesophageal dysmotility | 50% |
| Pulmonary hypertension | 10-25% |
| Renal disease | Rare (unlike SLE) |
| Test | Finding |
|---|---|
| ANA | Positive (speckled pattern) |
| Anti-U1 RNP | High titre (essential) |
| CK | Elevated if myositis |
| PFTs | Restrictive if ILD |
| Echo | PAH screening |
Algorithm
Symptom-Directed Treatment
| Manifestation | Treatment |
|---|---|
| Raynaud's | Calcium channel blockers, PDE5i |
| Arthritis | NSAIDs, DMARDs |
| Myositis | Steroids, azathioprine |
| ILD | Steroids, mycophenolate |
| PAH | ERA, PDE5i, prostanoids |
| Oesophageal | PPI, prokinetics |
-
Gunnarsson R et al. Mixed Connective Tissue Disease. Best Pract Res Clin Rheumatol. 2016;30(1):95-111. PMID: 27421218
-
Sharp GC et al. Mixed Connective Tissue Disease. Am J Med. 1972;52(2):148-159. PMID: 4621694
Viva Points
"MCTD is overlap syndrome with anti-U1 RNP. Features of SLE, scleroderma, polymyositis. Key manifestations: Raynaud's, swollen hands, myositis, ILD, PAH. Treatment is symptom-directed. Screen for PAH."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team