Systemic Mastocytosis
Summary
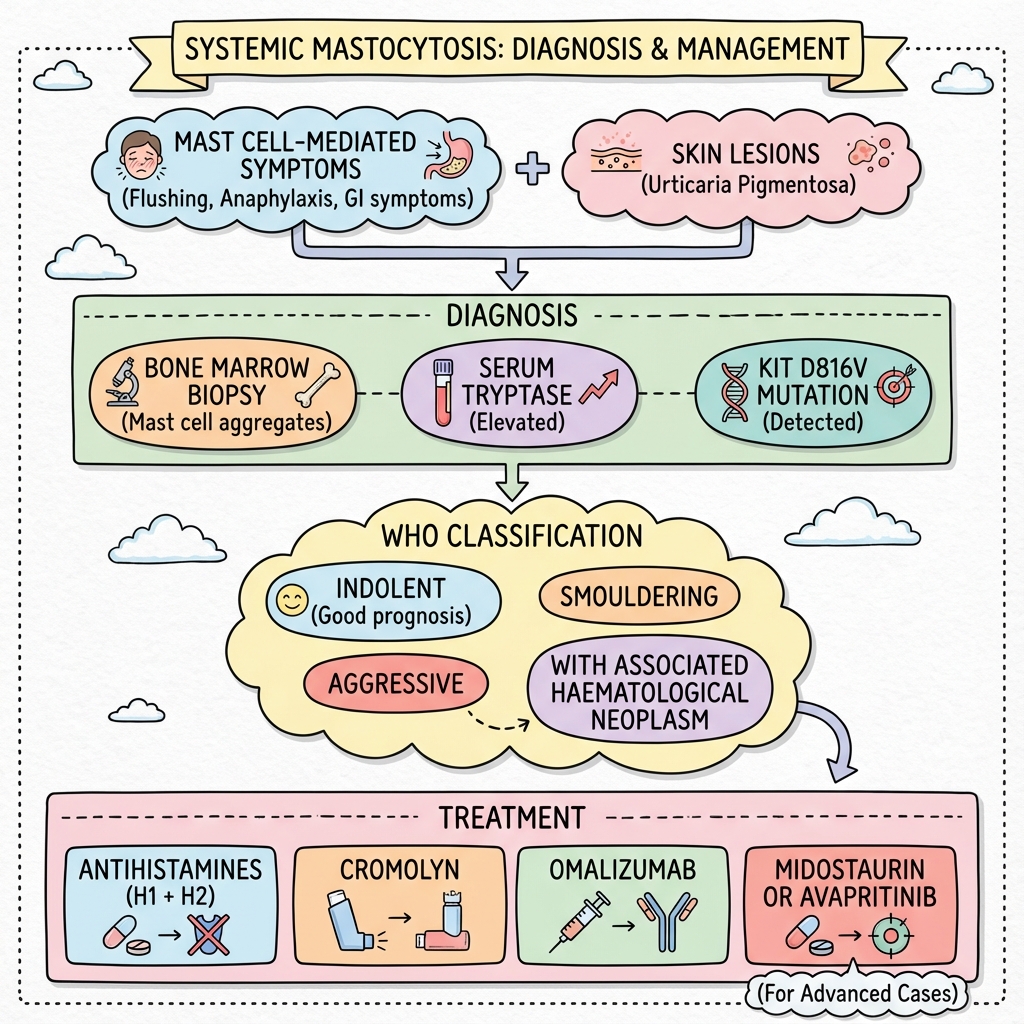
Systemic mastocytosis (SM) is a clonal mast cell disorder characterised by abnormal proliferation and accumulation of mast cells in tissues. It is associated with the KIT D816V mutation in greater than 90% of cases. Clinical manifestations result from mast cell mediator release (flushing, anaphylaxis, GI symptoms) and/or tissue infiltration (hepatosplenomegaly, cytopenias). Skin involvement (urticaria pigmentosa) is common but not universal. WHO classification ranges from indolent (good prognosis) to aggressive SM and mast cell leukaemia. Treatment focuses on symptom control (antihistamines) and targeted therapy (midostaurin, avapritinib) for advanced disease.
Key Facts
- Definition: Clonal mast cell accumulation in tissues
- Incidence: Rare; exact incidence unknown
- Peak Demographics: Adults; slight male predominance
- Pathognomonic: KIT D816V mutation + elevated tryptase + bone marrow mast cell aggregates
- Gold Standard Investigation: Bone marrow biopsy + KIT mutation + tryptase
- First-line Treatment: Antihistamines (H1+H2); targeted therapy for advanced
- Prognosis: Indolent SM - normal lifespan; aggressive - poor
Clinical Pearls
Diagnostic Pearl: Serum tryptase greater than 20 ng/mL is a minor WHO criterion; persistently elevated tryptase suggests mastocytosis.
Emergency Pearl: Patients with mastocytosis are at high risk of anaphylaxis - carry epinephrine.
Treatment Pearl: Avapritinib is highly effective for KIT D816V+ advanced SM.
Mast Cell Mediator Symptoms
Skin (Cutaneous Mastocytosis)
Organ Infiltration
| Subtype | Features |
|---|---|
| Indolent SM | No organ damage; good prognosis |
| Smouldering SM | Higher burden; close monitoring |
| Aggressive SM | Organ damage (C-findings) |
| SM-AHN | With associated haematological neoplasm |
| Mast cell leukaemia | High mast cell counts; poor prognosis |
| Test | Finding |
|---|---|
| Serum tryptase | Elevated (greater than 20 ng/mL) |
| Bone marrow biopsy | Mast cell aggregates; spindle-shaped |
| KIT D816V | Positive in greater than 90% |
| DEXA | Osteoporosis screening |
Algorithm
Symptom Control
| Drug | Notes |
|---|---|
| H1 antihistamine | Cetirizine, loratadine |
| H2 antihistamine | Famotidine, ranitidine |
| Cromolyn sodium | GI symptoms |
| Epinephrine | Emergency; carry autoinjector |
| Omalizumab | Refractory anaphylaxis |
Advanced Disease
| Drug | Evidence |
|---|---|
| Midostaurin | KIT inhibitor; approved for advanced SM |
| Avapritinib | Highly selective KIT D816V inhibitor |
| Cladribine | Cytoreductive |
-
Valent P et al. Mastocytosis: 2016 Updated WHO Classification and Novel Emerging Treatment Concepts. Blood. 2017;129(11):1420-1427. PMID: 28031187
-
Gotlib J et al. Efficacy and Safety of Midostaurin in Advanced Systemic Mastocytosis. N Engl J Med. 2016;374(26):2530-2541. PMID: 27355533
Viva Points
"Systemic mastocytosis is clonal mast cell disorder with KIT D816V. Diagnose with elevated tryptase, bone marrow aggregates, KIT mutation. Indolent = good prognosis. Treat symptoms with antihistamines; advanced disease with midostaurin/avapritinib."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team