Acute Ischaemic Stroke
Summary
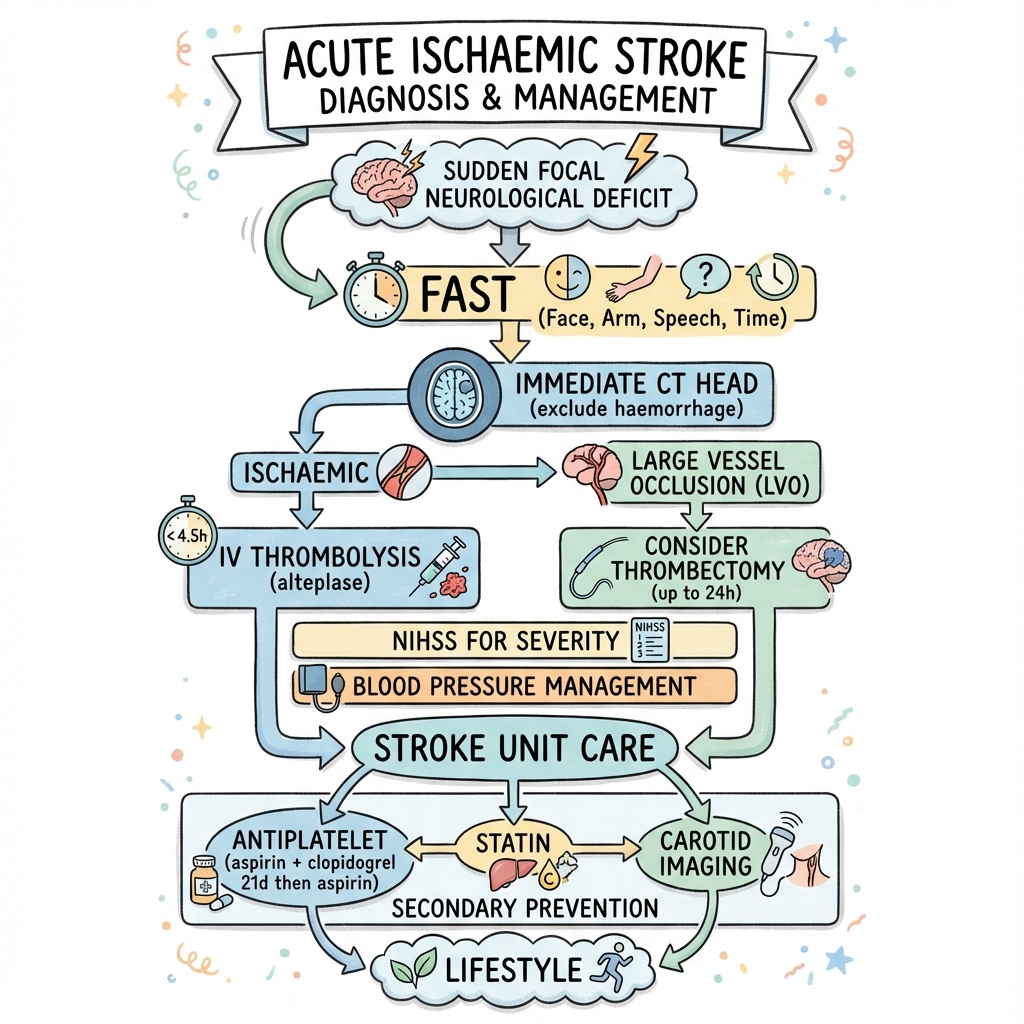
Acute ischaemic stroke is a neurological emergency caused by cerebral artery occlusion resulting in brain infarction. Rapid recognition using FAST (Face, Arm, Speech, Time) and immediate CT to exclude haemorrhage enables time-critical reperfusion therapy. IV thrombolysis (alteplase) within 4.5 hours and mechanical thrombectomy for large vessel occlusion up to 24 hours improve outcomes. Secondary prevention with antiplatelets, statins, and risk factor management reduces recurrence.
Key Facts
- Definition: Acute brain infarction from arterial occlusion
- Incidence: 150 per 100,000 per year
- Pathognomonic: Sudden focal neurological deficit + CT/MRI evidence
- Gold Standard Investigation: CT head (exclude bleed), CT angiography (LVO)
- First-line Treatment: IV alteplase within 4.5h; thrombectomy if LVO
- Prognosis: Without treatment 30% mortality; thrombolysis improves outcomes
Clinical Pearls
Time Pearl: Every 15-minute delay in thrombolysis reduces benefit.
NIHSS Pearl: Score greater than 6 with proximal occlusion = consider thrombectomy.
DAPT Pearl: Aspirin + clopidogrel for 21 days then aspirin alone for minor stroke/TIA.
Algorithm
Acute
| Time Window | Treatment |
|---|---|
| 0-4.5h | IV alteplase 0.9mg/kg (max 90mg) |
| 0-24h | Thrombectomy if LVO |
Secondary Prevention
| Intervention | Details |
|---|---|
| Antiplatelet | Aspirin 300mg then 75mg OD |
| Statin | Atorvastatin 80mg |
| BP control | After acute phase |
| Carotid imaging | Endarterectomy if stenosis 70%+ |
-
Powers WJ et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke. Stroke. 2019;50(12):e344-e418. PMID: 31662037
-
NICE guideline NG128. Stroke and transient ischaemic attack in over 16s. 2019.
Viva Points
"Stroke is time-critical. FAST recognition. CT to exclude bleed. Alteplase within 4.5h. Thrombectomy for LVO up to 24h. Secondary prevention: DAPT 21d, statin, BP, carotid."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team