Hyponatraemia
Summary
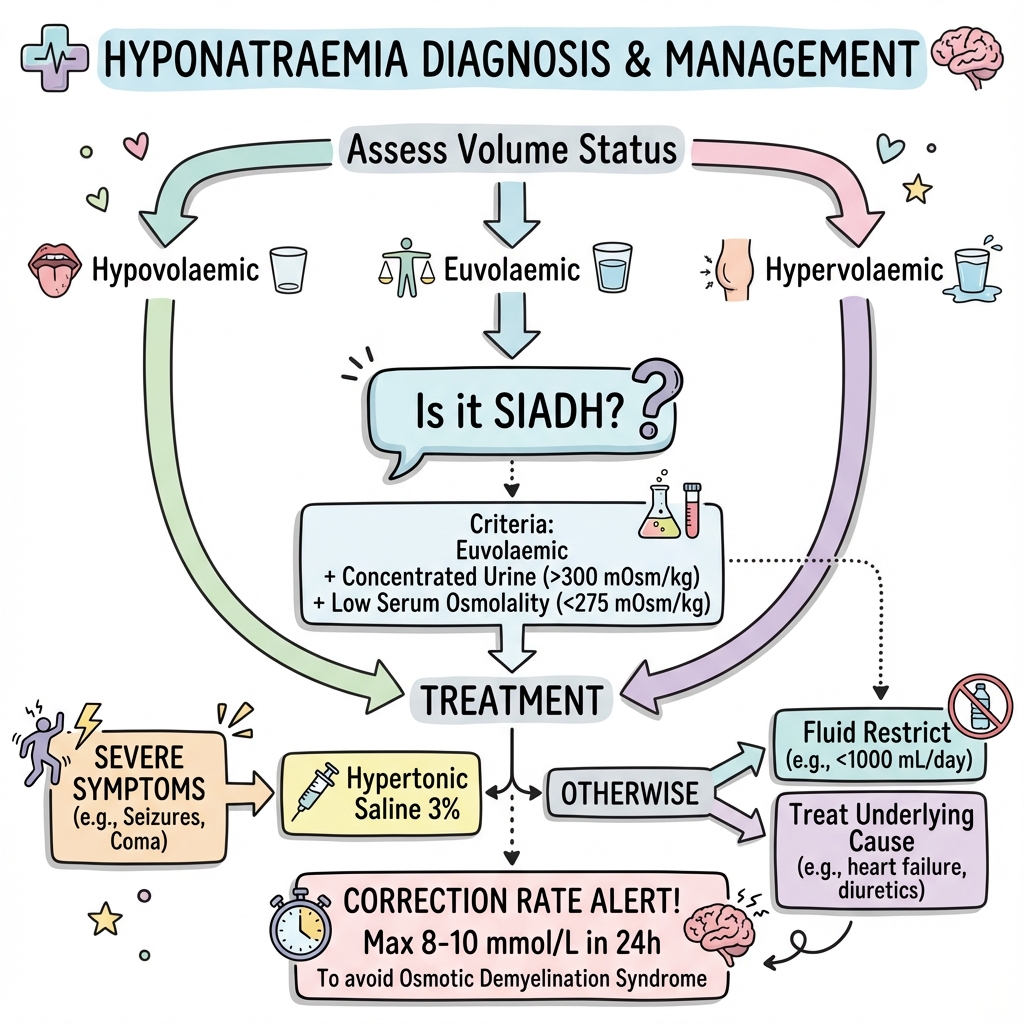
Hyponatraemia (serum Na+ less than 135 mmol/L) is the most common electrolyte disorder. Clinical assessment of volume status is key to diagnosis and management. SIADH (euvolaemic hyponatraemia) is a common cause. Severe symptomatic hyponatraemia requires urgent treatment with hypertonic saline, but correction must be slow (max 8-10 mmol/L in 24h) to avoid osmotic demyelination syndrome.
Key Facts
- Definition: Serum Na+ less than 135 mmol/L
- Incidence: 15-30% of hospitalised patients
- Pathognomonic: Low serum osmolality + assessment of volume status
- Gold Standard Investigation: Serum/urine osmolality, urine Na+
- First-line Treatment: Treat underlying cause; fluid restrict for SIADH
- Prognosis: Good if managed carefully; ODS if corrected too fast
Clinical Pearls
Volume Pearl: Assess volume status - hypovolaemic, euvolaemic, hypervolaemic.
SIADH Pearl: SIADH = euvolaemic + concentrated urine + low serum osmolality.
Correction Pearl: Never correct faster than 8-10 mmol/L in 24h - risk of ODS.
| Volume | Causes |
|---|---|
| Hypovolaemic | GI losses, diuretics, Addison's |
| Euvolaemic | SIADH, hypothyroidism, psychogenic polydipsia |
| Hypervolaemic | Heart failure, cirrhosis, nephrotic syndrome |
Algorithm
Symptomatic/Severe
| Intervention | Details |
|---|---|
| Hypertonic saline | 3% NaCl 100-150ml bolus |
| Target | Raise Na+ by 4-6 mmol in first hours |
SIADH
- Fluid restriction (750-1000ml/day)
- Treat underlying cause
- Vaptans (tolvaptan) if refractory
Correction Limits
- Maximum 8-10 mmol/L in 24h
- Maximum 18 mmol/L in 48h
- Spasovski G et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Eur J Endocrinol. 2014;170(3):G1-47. PMID: 24569125
Viva Points
"Hyponatraemia: assess volume status. SIADH = euvolaemic + concentrated urine. Severe symptoms = hypertonic saline. Correct slowly (8-10mmol/24h) to avoid ODS."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team