Giant Cell Arteritis
Summary
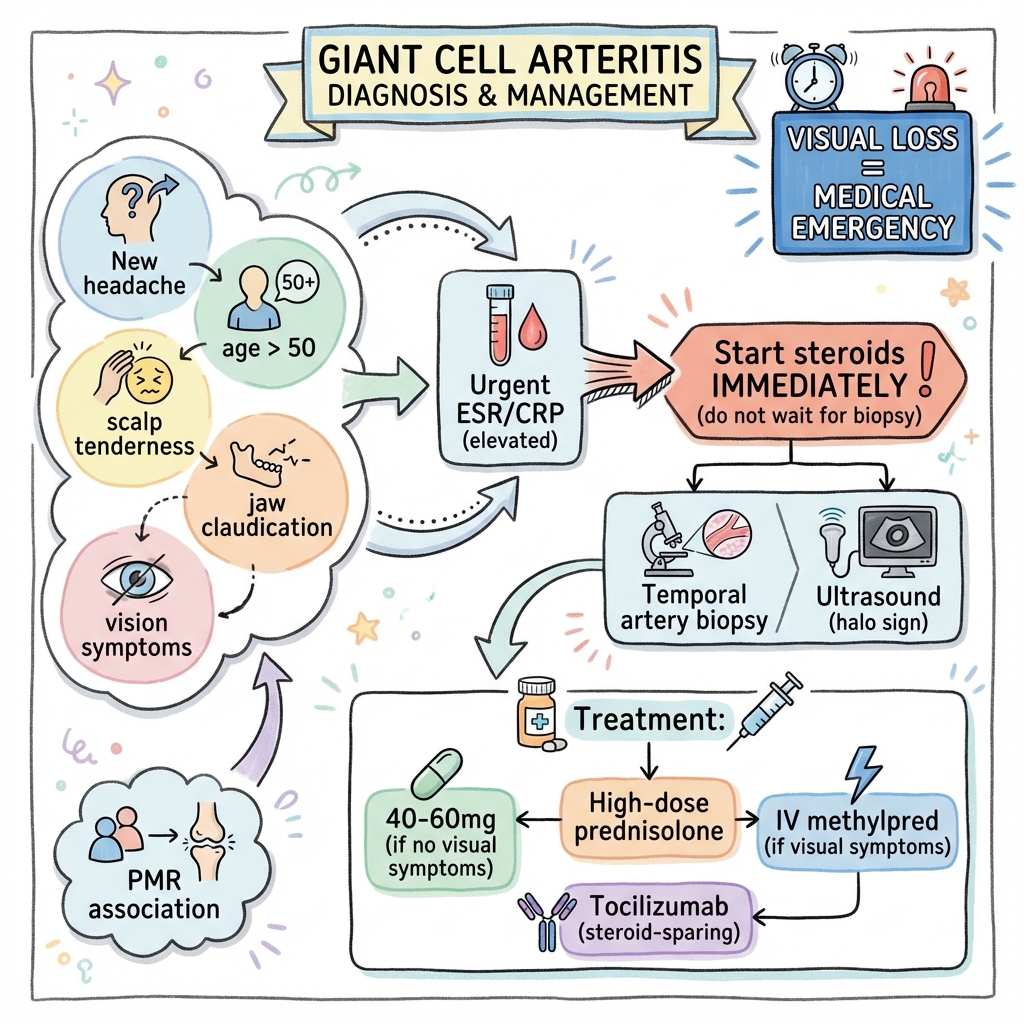
Giant cell arteritis (GCA) is a large-vessel vasculitis affecting predominantly the cranial arteries, particularly the temporal arteries. It is a medical emergency due to the risk of irreversible vision loss. GCA occurs almost exclusively in patients over 50 years and has a strong association with polymyalgia rheumatica (PMR). Classic features include new-onset headache, scalp tenderness, jaw claudication, and visual symptoms. Inflammatory markers (ESR, CRP) are markedly elevated. Steroids must be started immediately if suspected - do not wait for biopsy. Tocilizumab is now established as steroid-sparing therapy.
Key Facts
- Definition: Large-vessel vasculitis affecting cranial arteries
- Incidence: 15-25 per 100,000 in over 50s
- Peak Demographics: Age greater than 50; peak 70-80; F greater than M
- Pathognomonic: Temporal artery tenderness + jaw claudication + elevated ESR
- Gold Standard Investigation: Temporal artery biopsy or ultrasound (halo sign)
- First-line Treatment: High-dose prednisolone (40-60mg); IV methylpred if visual symptoms
- Prognosis: Excellent if treated early; permanent vision loss if delayed
Clinical Pearls
Emergency Pearl: Visual loss in GCA can be irreversible within hours. Start steroids immediately if suspected.
Diagnostic Pearl: Biopsy remains positive for 2-4 weeks after starting steroids - do not delay treatment.
Treatment Pearl: Tocilizumab (GiACTA trial) reduces relapse and steroid exposure.
Symptoms
Signs
Red Flags
[!CAUTION]
- Any visual symptoms = emergency
- Jaw claudication
- Sudden vision loss
| Test | Finding |
|---|---|
| ESR | Markedly elevated (often greater than 50) |
| CRP | Elevated |
| Temporal artery biopsy | Giant cells, intimal hyperplasia, skip lesions |
| Ultrasound | Halo sign (dark rim around vessel) |
| CT/MR angiography | Large vessel involvement |
Algorithm
Immediate Treatment
| Scenario | Treatment |
|---|---|
| GCA without visual symptoms | Prednisolone 40-60mg daily |
| GCA with visual symptoms | IV methylprednisolone 500mg-1g daily x3, then oral |
Steroid Taper
- Slow taper over 12-24 months
- Monitor symptoms and inflammatory markers
Steroid-Sparing
| Drug | Evidence |
|---|---|
| Tocilizumab | GiACTA trial; weekly or fortnightly SC |
Adjuncts
- Aspirin 75mg (controversial but often used)
- Bone protection (bisphosphonates, calcium, vitamin D)
- PPI
-
BSR/BHPR Guidelines for the Management of Giant Cell Arteritis. Rheumatology. 2020. PMID: 32134455
-
Stone JH et al. Trial of Tocilizumab in Giant-Cell Arteritis (GiACTA). N Engl J Med. 2017;377(4):317-328. PMID: 28745999
Viva Points
"GCA is large-vessel vasculitis in over 50s. Presents with headache, jaw claudication, visual symptoms. Visual loss is an emergency. Start steroids immediately. Tocilizumab (GiACTA) is steroid-sparing."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team