Crohn's Disease
Summary
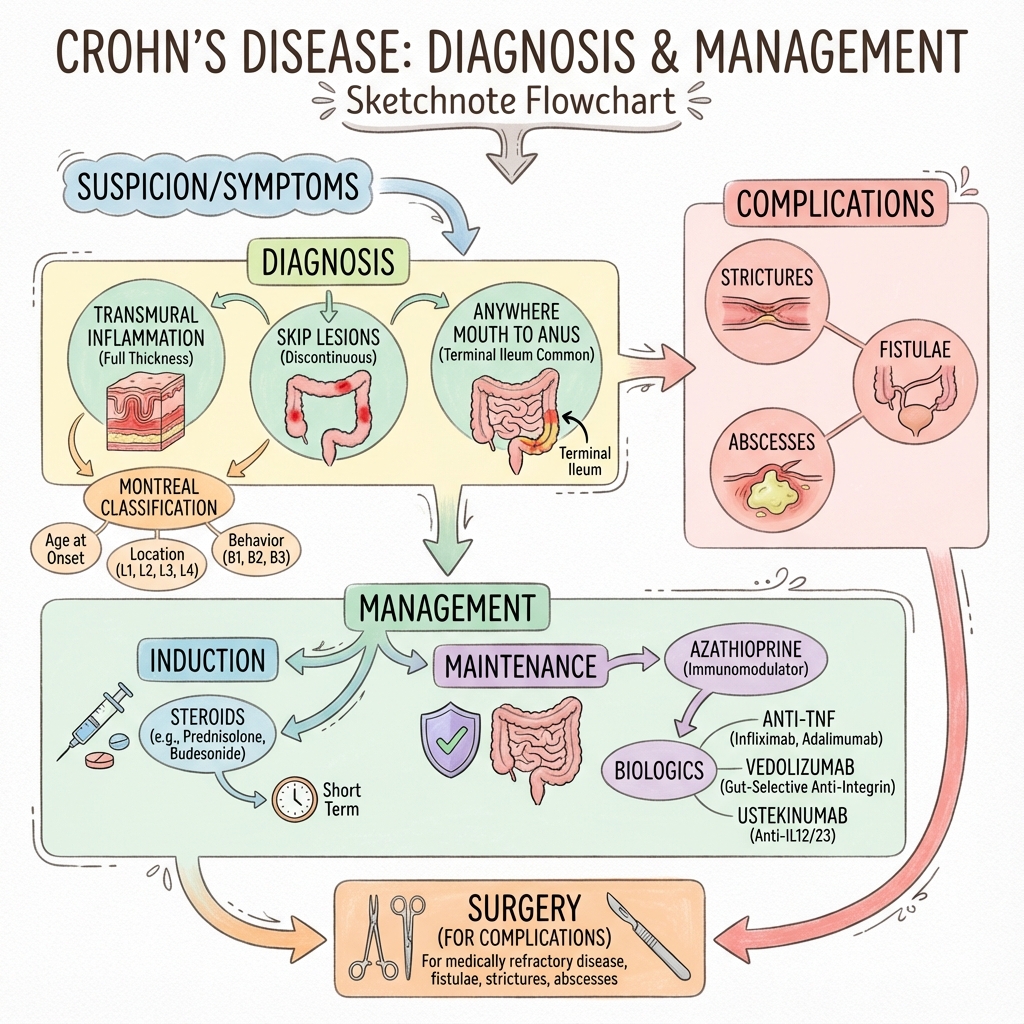
Crohn's disease is a chronic inflammatory bowel disease characterised by transmural inflammation that can affect any part of the GI tract from mouth to anus, most commonly the terminal ileum. It causes skip lesions, strictures, and fistulae. Treatment involves induction of remission (steroids) followed by maintenance therapy (immunomodulators, biologics). Surgery is reserved for complications.
Key Facts
- Definition: Chronic transmural granulomatous inflammation of GI tract
- Incidence: 3-20 per 100,000 per year
- Pathognomonic: Skip lesions + transmural inflammation + granulomas
- Gold Standard Investigation: Colonoscopy + biopsy + imaging
- First-line Treatment: Steroids for induction; azathioprine/biologics for maintenance
- Prognosis: Chronic relapsing; 50% need surgery within 10 years
Clinical Pearls
Distribution Pearl: Terminal ileum most common; can be anywhere mouth to anus.
Fistula Pearl: Crohn's causes fistulae (entero-enteric, perianal) - UC doesn't.
Biologic Pearl: Anti-TNF, vedolizumab, ustekinumab all effective for moderate-severe.
| Location | Distribution |
|---|---|
| L1 | Terminal ileum |
| L2 | Colon |
| L3 | Ileocolonic |
| L4 | Upper GI |
| Behaviour | |
|---|---|
| B1 | Non-stricturing, non-penetrating |
| B2 | Stricturing |
| B3 | Penetrating |
Algorithm
Induction
| Severity | Treatment |
|---|---|
| Mild | Budesonide (ileal) |
| Moderate-severe | Prednisolone 40mg |
Maintenance
| Drug | Notes |
|---|---|
| Azathioprine | First-line steroid-sparing |
| Anti-TNF | Infliximab, adalimumab |
| Vedolizumab | Gut-selective integrin |
| Ustekinumab | IL-12/23 |
-
Torres J et al. Crohn's disease. Lancet. 2017;389(10080):1741-1755. PMID: 27914655
-
NICE guideline NG129. Crohn's disease: management. 2019.
Viva Points
"Crohn's: transmural, skip lesions, terminal ileum, fistulae. Steroids to induce. Azathioprine or biologics for maintenance. Surgery for complications."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team