Chronic Kidney Disease
Summary
Chronic kidney disease (CKD) is sustained reduction in kidney function defined by eGFR less than 60 or markers of kidney damage for 3+ months. It is staged by GFR (G1-G5) and albuminuria (A1-A3). Common causes are diabetes and hypertension. Management focuses on BP control (ACEi/ARBs), glycaemic control, SGLT2 inhibitors, and avoiding nephrotoxins. Preparation for renal replacement therapy (dialysis, transplant) or conservative care is required for advanced CKD.
Key Facts
- Definition: eGFR less than 60 or kidney damage for 3+ months
- Incidence: 10-15% of adults
- Pathognomonic: Reduced eGFR + albuminuria
- Gold Standard Investigation: eGFR + uACR
- First-line Treatment: ACEi/ARB + SGLT2 inhibitor
- Prognosis: Progressive; RRT if stage 5
Clinical Pearls
ACEi Pearl: ACEi/ARBs slow progression - tolerate up to 25% creatinine rise.
SGLT2 Pearl: SGLT2 inhibitors reduce CKD progression independent of diabetes.
Finerenone Pearl: MRA (finerenone) now evidence-based for diabetic CKD.
| Stage | GFR | Description |
|---|---|---|
| G1 | 90+ | Normal/high |
| G2 | 60-89 | Mildly decreased |
| G3a | 45-59 | Mild-moderately decreased |
| G3b | 30-44 | Moderate-severely decreased |
| G4 | 15-29 | Severely decreased |
| G5 | less than 15 | Kidney failure |
Algorithm
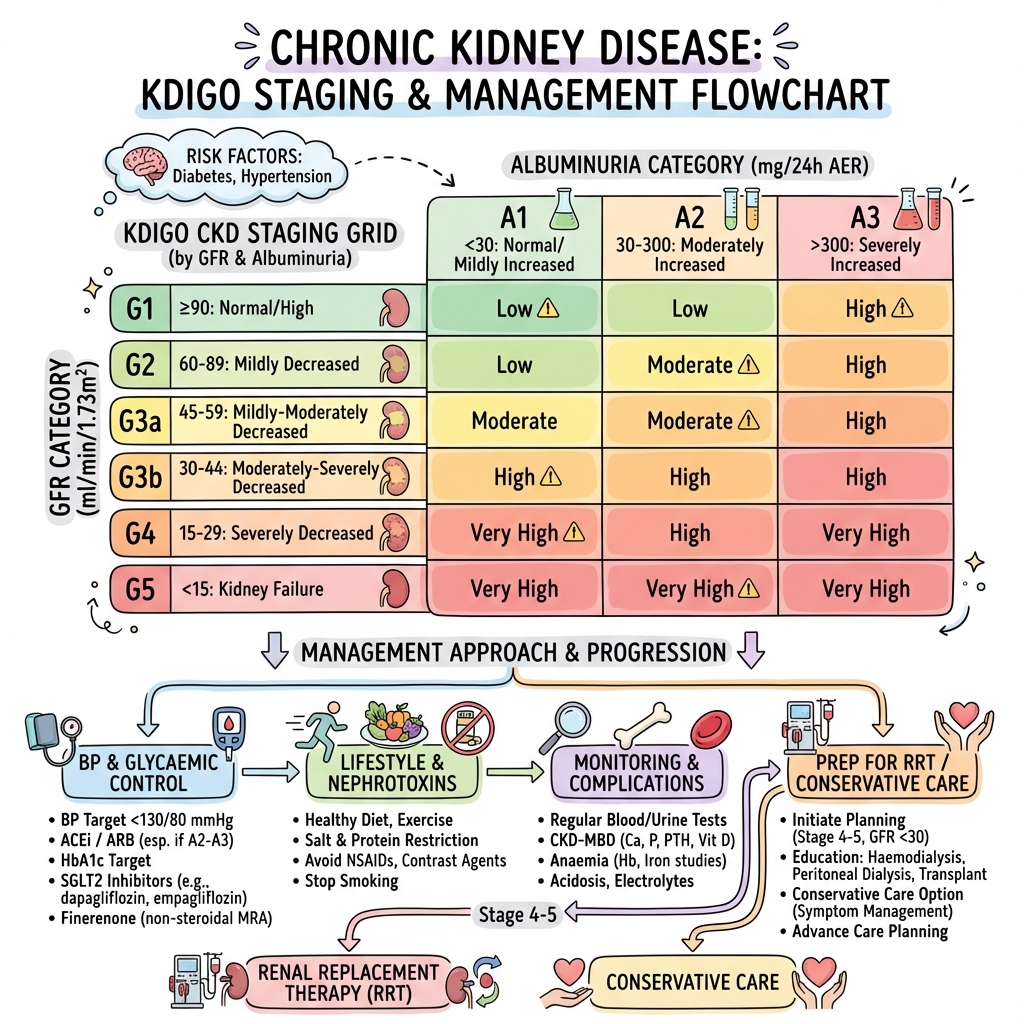
Key Interventions
| Intervention | Details |
|---|---|
| BP | ACEi or ARB; target less than 130/80 |
| Diabetes | SGLT2 inhibitor + optimise HbA1c |
| Finerenone | If diabetic CKD |
| Lifestyle | Low salt, stop smoking |
| Avoid | NSAIDs, nephrotoxins |
CKD Complications
- CKD-MBD: phosphate binders, vitamin D
- Anaemia: Iron, ESAs
- Acidosis: Bicarbonate
-
KDIGO. Clinical Practice Guideline for the Evaluation and Management of CKD. 2024.
-
NICE guideline NG203. Chronic kidney disease. 2021.
Viva Points
"CKD: stage by GFR and albuminuria. ACEi/ARB + SGLT2i for all. SGLT2i protects kidneys. Prepare for RRT at G4-5."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team