Acute Pancreatitis
Summary
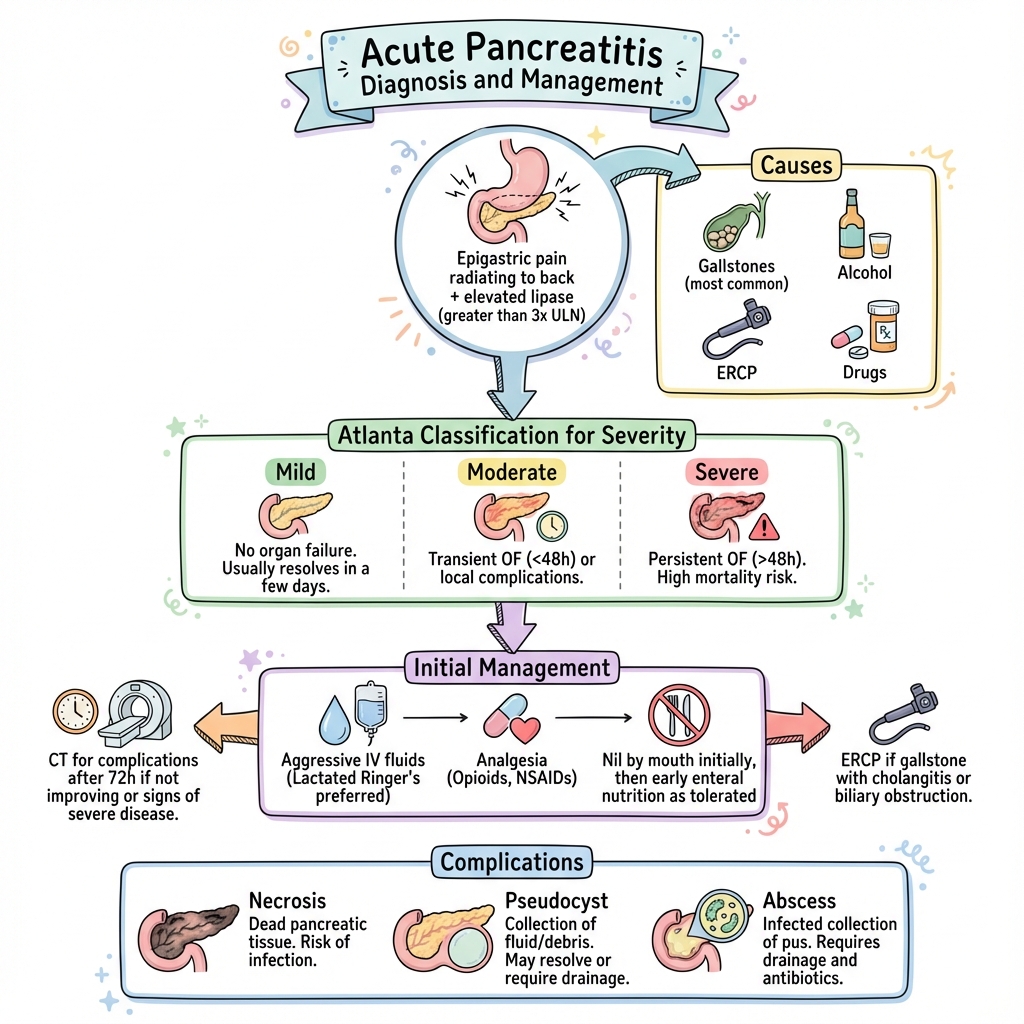
Acute pancreatitis is an inflammatory condition of the pancreas ranging from mild oedematous disease to severe necrotising pancreatitis with multi-organ failure. Gallstones and alcohol account for 80% of cases. Diagnosis requires 2 of 3 criteria: characteristic abdominal pain, lipase greater than 3x upper limit of normal, and imaging findings. Severity is classified by the revised Atlanta criteria based on organ failure. Management is supportive with aggressive IV fluids, analgesia, and early enteral nutrition. ERCP is indicated for gallstone pancreatitis with biliary obstruction or cholangitis.
Key Facts
- Definition: Acute inflammation of the pancreas
- Incidence: 30-40 per 100,000 per year
- Peak Demographics: Gallstone (older women), Alcohol (middle-aged men)
- Pathognomonic: Epigastric pain + lipase greater than 3x ULN
- Gold Standard Investigation: Lipase/amylase; CT if complications suspected
- First-line Treatment: IV fluids, analgesia, early nutrition
- Prognosis: Mild 1% mortality; severe 30% mortality
Clinical Pearls
Diagnostic Pearl: Lipase is more sensitive and specific than amylase.
Fluid Pearl: Goal-directed fluid resuscitation in first 24h is critical - aim for adequate urine output.
Nutrition Pearl: Early enteral nutrition (within 24-48h) is recommended over prolonged nil by mouth.
| Cause | Frequency |
|---|---|
| Gallstones | 40% |
| Alcohol | 30-40% |
| Idiopathic | 10-15% |
| ERCP | 5% |
| Drugs | Rare |
| Hypertriglyceridaemia | Rare |
| Hypercalcaemia | Rare |
| Severity | Definition |
|---|---|
| Mild | No organ failure, no local complications |
| Moderately severe | Transient organ failure (less than 48h) or local complications |
| Severe | Persistent organ failure (greater than 48h) |
Algorithm
Initial Management
| Intervention | Details |
|---|---|
| IV fluids | Lactated Ringer's, goal-directed |
| Analgesia | Opioids (morphine safe) |
| Nil by mouth | Initially, then early enteral nutrition |
| Monitoring | ICU if severe |
Specific
| Scenario | Management |
|---|---|
| Gallstone + cholangitis | Urgent ERCP |
| Gallstone (no cholangitis) | Cholecystectomy this admission |
| Infected necrosis | Antibiotics, step-up drainage |
-
Banks PA et al. Classification of acute pancreatitis - 2012 Revision of Atlanta Classification. Gut. 2013;62(1):102-111. PMID: 23100216
-
IAP/APA Guidelines. Evidence-based guidelines for the management of acute pancreatitis. Pancreatology. 2013;13(4 Suppl 2):e1-15. PMID: 24054878
Viva Points
"Acute pancreatitis: gallstones or alcohol. Diagnose with lipase greater than 3x ULN. Atlanta classification: mild/moderate/severe based on organ failure. Aggressive fluids, early enteral nutrition, ERCP for cholangitis."
Last Reviewed: 2026-01-01 | MedVellum Editorial Team